Upper limb fractures and shoulder injuries commonly occur following falls, sporting injuries, workplace accidents, motor vehicle accidents, or other forms of trauma. These injuries can affect the bones, joints, and supporting structures of the shoulder, upper arm, elbow, forearm, and wrist, often causing significant pain, swelling, weakness, and difficulty using the arm.
Some injuries occur after a high-impact event, while others may result from a simple fall onto an outstretched hand or direct impact to the shoulder or arm. In older adults, fractures can sometimes occur more easily due to reduced bone strength or osteoporosis.
The severity of upper limb injuries can vary from stable fractures managed with immobilisation and rehabilitation through to more complex injuries that may require surgical treatment to restore alignment, stability, and function.
Dr Scott Tulloch consults for a range of upper limb fractures and traumatic shoulder injuries, which are outlined in further detail below. Treatment recommendations are tailored to the specific injury pattern, severity of the fracture or injury, functional requirements, and overall health of each patient.

A distal radius fracture, commonly referred to as a wrist fracture, occurs when the radius bone near the wrist breaks. These injuries commonly happen after a fall onto an outstretched hand, although they can also occur during sporting injuries, cycling accidents, workplace trauma, or motor vehicle accidents. In older adults, wrist fractures may occur more easily due to reduced bone density or osteoporosis.
Symptoms often include pain, swelling, bruising, reduced wrist movement, weakness, or visible deformity around the wrist. If a wrist fracture is suspected, it is important to seek prompt medical assessment. Initial management may include resting the arm, applying ice, elevating the wrist, and avoiding further use of the hand or wrist until the injury has been assessed.
Diagnosis is typically made through a combination of clinical examination and imaging, most commonly X-rays. In some cases, additional imaging such as a CT scan may be recommended to assess fracture complexity or joint involvement.
Treatment depends on factors such as the type of fracture, degree of displacement, joint involvement, bone quality, and functional demands of the patient. Some fractures can be managed with immobilisation in a cast or splint, while more unstable or displaced fractures may require surgical stabilisation using plates, screws, or pins to restore alignment and support healing.
Rehabilitation and physiotherapy are often important parts of recovery, helping restore movement, strength, and wrist function following healing.

Forearm and elbow fractures can occur following falls, sporting injuries, workplace accidents, motor vehicle accidents, or direct trauma to the arm. These injuries may involve the bones of the forearm (radius and ulna) or the bones that form the elbow joint, and can range from relatively simple fractures through to more complex injuries involving the joint surface or surrounding ligaments.
Symptoms commonly include pain, swelling, bruising, reduced movement, weakness, or visible deformity around the forearm or elbow. In some cases, patients may experience difficulty rotating the forearm, bending the elbow, or using the arm for everyday activities. If a fracture is suspected, it is important to seek prompt medical assessment. Initial care may include resting the arm, applying ice, elevating the limb, and using a sling or splint to minimise movement until the injury is assessed.
Diagnosis is typically made through a combination of clinical examination and imaging, most commonly X-rays. In more complex injuries, additional imaging such as a CT scan may be recommended to better assess fracture alignment, joint involvement, or associated injuries.
Treatment depends on the location and severity of the fracture, degree of displacement, joint stability, and overall functional requirements of the patient. Some fractures can be managed with immobilisation in a cast or brace, while more unstable or displaced injuries may require surgical treatment to restore alignment and joint function. Rehabilitation and physiotherapy are often important parts of recovery, helping restore movement, strength, and arm function following healing.

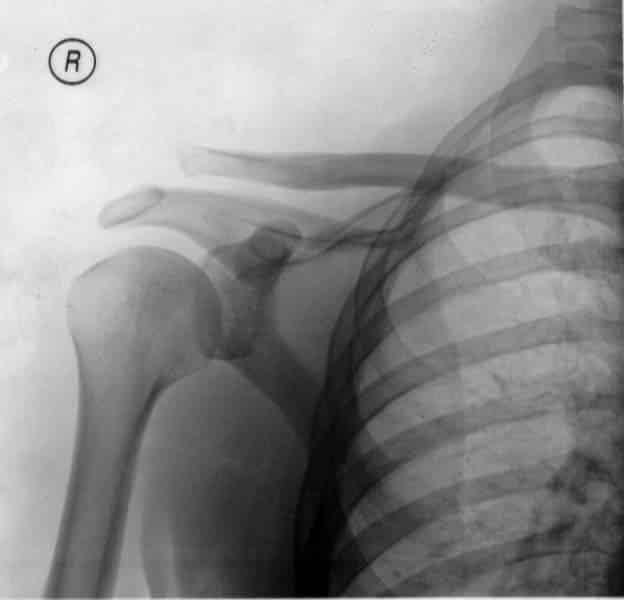
Shoulder fractures involve a break in one of the bones around the shoulder joint, most commonly the proximal humerus (upper arm bone), although fractures can also involve the shoulder blade or surrounding structures. These injuries commonly occur following falls, sporting injuries, cycling accidents, motor vehicle accidents, or direct trauma to the shoulder. In older adults, shoulder fractures may occur more easily due to reduced bone density or osteoporosis.
Symptoms often include pain, swelling, bruising, difficulty moving the arm, weakness, or visible deformity around the shoulder. Many patients find it difficult to lift the arm or perform everyday activities following the injury. If a shoulder fracture is suspected, it is important to seek prompt medical assessment. Initial management may include supporting the arm in a sling, applying ice, and avoiding further movement until the injury has been assessed.
Diagnosis is typically made through a combination of clinical examination and imaging, most commonly X-rays. In some cases, additional imaging such as a CT scan may be recommended to better assess fracture complexity, displacement, or joint involvement.
Treatment depends on factors such as the type of fracture, degree of displacement, bone quality, and overall functional requirements of the patient. Some shoulder fractures can be managed with immobilisation in a sling followed by rehabilitation, while more complex or displaced fractures may require surgical treatment to restore alignment and shoulder function. Physiotherapy is often an important part of recovery, helping restore movement, strength, and shoulder mobility following healing.

Clavicle fractures, commonly known as collarbone fractures, are common upper limb injuries that occur when the clavicle bone breaks. These fractures often result from falls onto the shoulder, sporting injuries, cycling accidents, or direct impact to the upper chest or shoulder region.
Symptoms commonly include pain, swelling, bruising, and difficulty moving the arm or shoulder. Some patients may notice a visible bump or deformity along the collarbone. Movements involving lifting the arm or reaching overhead are often painful following the injury. If a clavicle fracture is suspected, it is important to seek prompt medical assessment. Initial care may include supporting the arm in a sling, applying ice, and avoiding activities that place stress on the shoulder.
Diagnosis is typically made through a combination of clinical examination and X-rays to assess the location and alignment of the fracture. In some cases, additional imaging may be required to evaluate more complex injuries or associated shoulder trauma.
Treatment depends on factors such as the location of the fracture, degree of displacement, shortening of the bone, activity level, and overall functional requirements of the patient. Many clavicle fractures can be managed with immobilisation in a sling and rehabilitation, allowing the bone to heal naturally over time. More displaced or unstable fractures may require surgical stabilisation using plates and screws to restore alignment and shoulder function.
Rehabilitation and physiotherapy are often important parts of recovery, helping restore movement, strength, and shoulder function following healing.

Humerus fractures involve a break in the upper arm bone (humerus) and can occur near the shoulder, through the shaft of the bone, or closer to the elbow. These injuries commonly result from falls, sporting injuries, motor vehicle accidents, workplace trauma, or direct impact to the arm. In older adults, fractures may occur more easily due to reduced bone density or osteoporosis.
Symptoms often include pain, swelling, bruising, weakness, reduced arm movement, or visible deformity. Many patients find it difficult to lift or use the arm following the injury. Depending on the location and severity of the fracture, there may also be associated irritation to nearby nerves or soft tissues. If a humerus fracture is suspected, it is important to seek prompt medical assessment. Initial management may include supporting the arm in a sling, applying ice, and avoiding further movement until the injury has been assessed.
Diagnosis is typically made through a combination of clinical examination and imaging, most commonly X-rays. In some cases, additional imaging such as a CT scan may be recommended to better assess fracture complexity, displacement, or joint involvement.
Treatment depends on factors such as the location and pattern of the fracture, degree of displacement, bone quality, and functional requirements of the patient. Some humerus fractures can be managed with immobilisation and rehabilitation, while more unstable or displaced fractures may require surgical treatment to restore alignment and support healing.
Rehabilitation and physiotherapy are often important parts of recovery, helping restore movement, strength, and arm function following healing.

Acromioclavicular (AC) joint injuries occur when the joint at the top of the shoulder, where the collarbone (clavicle) meets the shoulder blade (acromion), is injured or disrupted. These injuries commonly result from falls directly onto the shoulder, sporting collisions, cycling accidents, or other traumatic impacts.
AC joint injuries can range from mild sprains of the supporting ligaments through to more significant injuries where the collarbone becomes displaced. Symptoms commonly include pain at the top of the shoulder, swelling, bruising, weakness, and difficulty lifting or moving the arm. In more severe injuries, a visible bump may develop over the collarbone due to displacement of the joint.
Diagnosis is typically made through a combination of clinical examination and X-rays to assess the degree of joint separation and identify any associated fractures or injuries. In some cases, additional imaging may be recommended if there is concern about associated soft tissue damage or shoulder instability.
Treatment depends on the severity of the injury, degree of displacement, symptoms, activity level, and functional requirements of the patient. Many AC joint injuries can be managed with rest, ice, sling immobilisation, and physiotherapy, allowing the ligaments to heal over time. More severe or unstable injuries, particularly in active individuals, may require surgical stabilisation to restore joint alignment and shoulder function.
Rehabilitation and physiotherapy are important parts of recovery, helping restore movement, strength, and shoulder stability following healing.